How accurate is the US coronavirus death count? Some experts say it's off by 'tens of thousands'
To get an accurate picture of the pandemic, US needs to test more of the dead.
The novel coronavirus has already claimed the lives of more than 61,000 Americans. But experts fear that number could be far higher at this point in the outbreak -- perhaps by 50% -- once the pandemic subsides enough for officials to go back and make a true reckoning of the dead.
Experts are urging leaders to take measures right now to preserve data and medical specimens so that science has the chance to determine the precise number of people who succumbed during one of the most severe global pandemics in memory.
"Under-counting deaths in this particular epidemic is happening all over," said Dr. Daniel Lopez-Acuna, an epidemiologist and former top World Health Organization official, who spent 30 years at the organization. "It’s almost inevitable."
Tune into ABC at 1 p.m. ET and ABC News Live at 4 p.m. ET every weekday for special coverage of the novel coronavirus with the full ABC News team, including the latest news, context and analysis.
Calculating the precise number of COVID-19 deaths is remarkably complicated for a number of reasons. But leading epidemiologists, pathologists, medical examiners, medical history professors and local, state, federal and global health officials told ABC News that more testing is the single most important factor in determining an accurate national death count.
"We need to have the testing available because the big question now with COVID-19 is the denominator -- of anything," said Dr. Alex Williamson of the College of American Pathologists. "How many people get it? How many people recover? How many are hospitalized? How many died? We don't know the true denominator. More testing is the most important thing we need to do."

Ongoing testing kit shortages in cities and states nationwide means that only clearly symptomatic patients are currently being tested in many places. There also is no uniform national system in the U.S. for investigating deaths, and until two weeks ago, the U.S. was only counting Americans who lab-tested positive, before or after death, for COVID-19.
Left out of the tally are people who died without being tested and those who died at home or some other non-healthcare facilities before they could seek medical care.
"It is an extraordinary challenge," said Dr. Sally Aiken, president of the National Association of Medical Examiners. "There just isn't really the infrastructure."
Further undermining an accurate national count are new analyses that suggest the virus was spreading in the U.S. much earlier than previously believed, likely playing a role in more deaths than currently known.
California’s first known COVID-19 death to date was Patricia Cabello Dowd, 57, in Santa Clara County. Dowd died on Feb. 6 of heart complications, which were later determined to have been unleashed by the COVID-19 virus. Dowd's death -- in which an autopsy obtained by the San Francisco Chronicle listed a heart rupture "due to Covid-19 infection" -- came three weeks before the earliest previously identified American coronavirus-related death.
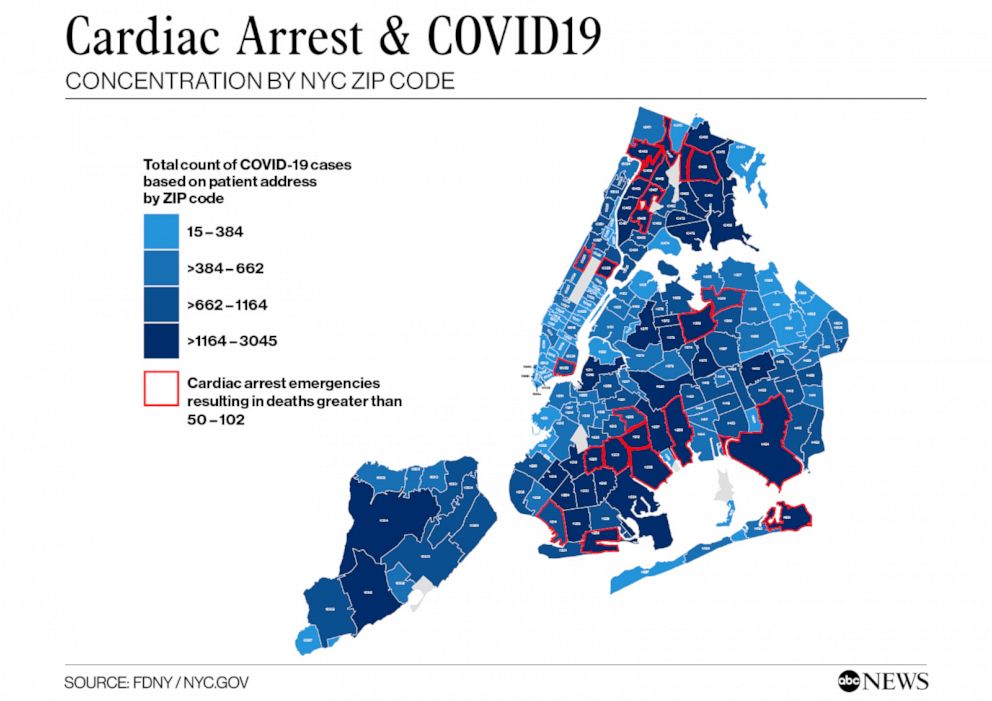
New data on cardiac arrest emergency calls reviewed by ABC News suggests that New York City’s catastrophic outbreak likely began in close-knit neighborhoods in Queens and Brooklyn as far back as mid-February.
Finally, as the cardiac arrest data suggested, scientists are contending with an ever-evolving understanding of how COVID-19 attacks the body. Initially, it was believed to primarily attack the lungs, but new research suggests it’s a danger to nearly every organ.
Experts say that many people like Dowd, who died of a nonrespiratory COVID-19 complication early in the outbreak -- before the pandemic’s impact became apparent -- may never be accurately counted.
The confusion and complications inherent in tracking pandemics have left a weary nation wondering just how high the actual U.S. death count may be -- and how bad things really are.
Less than 2% of all Americans have been tested for the coronavirus to date, according to White House figures -- nearly 5.5 million people. It's a figure that experts say is both higher than most nations and far lower per capita than where the U.S. should be at this point.
U.S. Assistant Secretary for Health and White House "testing czar" Admiral Brett Giroir told George Stephanopoulos on "Good Morning America" on Tuesday that the Trump administration doesn’t concur with a Harvard University study which concluded last week that the U.S. needs to be testing 5 million people a day in June and up to 20 million by July in order to safely re-open the country.
"We don’t believe those estimates are accurate, nor are they reasonable, " Giroir said.
Yet either way, that testing is still mostly focused on the living. Experts told ABC News that an accurate death toll is not only important to later get a better picture of what happened, but if possible, real-time or near real-time death counts can also help public health officials in their battle to contain the virus now.
History: A chilling guide
Researchers retrospectively calculate overall deaths from a pandemic by studying excess deaths year-to-year in a given region. But that’s a difficult figure to gauge until a pandemic is over.
Previous studies of other recent virus outbreaks suggest the actual number of COVID-19 deaths to date is very likely dramatically higher than the more than 60,000 deaths currently reported.
A Centers for Disease Control and Prevention (CDC) analysis of the H1N1 swine flu virus outbreak in the U.S. in 2009 and 2010 concluded two years later that the actual tally was likely 15 times higher than the officially recorded figures. A 2013 study by the U.S. National Institutes of Health determined the figure was seven times higher than the official count.
What to know about coronavirus:
- How it started and how to protect yourself: Coronavirus explained
- What to do if you have symptoms: Coronavirus symptoms
- Tracking the spread in the U.S. and worldwide: Coronavirus map
But scientists said that the current coronavirus pandemic is of an entirely different magnitude.
"I’ve never – none of us have ever – seen an infection like COVID-19, that literally stopped the world," said Williamson.
While most news organizations rely on the Johns Hopkins University figures, which are pulled directly from state and local government websites and are considered more timely picture of the problem, the National Center for Health Statistics (NCHS), a branch of the CDC, is the primary agency responsible for U.S. health statistics, which are compiled by collecting data on births, deaths and health surveys.
Due to the lack of a uniform U.S. system, the NCHS system lags about two weeks behind in reporting said, Dr. Robert Anderson, chief of mortality statistics. On May 1, the CDC acknowledged in a bulletin that nearly 40% of U.S. deaths are still not being reported to the federal agency within ten days.
Daniel Weinberger, an epidemiologist from the Yale School of Public Health, analyzed NCHS death count data to estimate how many COVID-19 deaths may have gone uncounted from March 1 to April 11.
He concluded the official death toll in the U.S. is "probably a substantial underestimate of the true number."

The actual figure, he said, may be "1.5 times higher."
The NCHS reports 23,500 COVID deaths in the 6 week period from March 1 to April 11. But Yale researchers analyzing publicly available mortality data report to ABC News found the country saw 36,000 more deaths than would normally be expected this time of year, suggesting the COVID death count could be around 1.5 times higher than what is being officially reported.
“The data on deaths for March and early April continue to fill in, so we are now getting a more complete picture of the early toll of the epidemic," Weinberger said. "As we get more data from the period when the epidemic was accelerating, these numbers will continue to climb sharply.”
Given the still-looming threat to the U.S., researchers are urging municipalities to maintain as much detailed data about COVID-19 records as possible.
With patchwork of reporting protocols, a 'pipe dream' to gauge actual death toll
As the pandemic rages across all 50 states and around the globe with no uniform reporting protocol in place, experts said the official death count is hard to even estimate.
"One of the difficulties is that every state does things differently," said William Hanage, an epidemiologist at Harvard University’s T.H. Chan School of Public Health. "When I look at the data, I’m sitting there thinking, ‘Okay, this is Oklahoma. What kind of modifier am I adding to that to figure out what’s going on here?’ It would be incredibly helpful not to have to do that."
He’s doubtful that a uniform national death count reporting process is possible anytime soon.
"It’s a bit of pipe dream," he said.

And that's before taking into account the ways other countries count their own death tolls.
"Even now if you’re comparing reporting among different countries, you’ve got to ask, ‘Are they reporting only deaths in hospitals? Only people they are sure had COVID? Which test did they use? What about deaths occurring elsewhere – in nursing homes and at home? Are they being counted?’"
COVID-19-related deaths in non-hospital settings -- largely nursing home deaths and deaths at home -- are also fueling revised death counts in some U.S. regions and nations around the world.
As many as half of the COVID-19 deaths in Europe may have come from nursing homes, Hans Kluge, the WHO's regional European director, said in a press briefing last week. When France added nursing homes to its tally, the nation’s death count spiked 40%, according to The Wall Street Journal.
While the U.S. is not currently counting nursing home deaths nationally, it’s estimated that thousands have died from or with COVID-19 complications in these facilities across the U.S. Last week ABC News reported that based on the reporting of 28 states, the death toll in long-term care facilities has already surged past 10,000.
Yet it was also only last week that the CDC began the laborious process of preparing to incorporate nursing home deaths into its overall death count. The agency issued a notification saying it would soon begin requiring that nursing homes report communicable disease deaths promptly to federal authorities. It’s unclear when the U.S. will begin including those figures in its national death count.
On April 14, the CDC directed all U.S. states and territories to begin counting suspected as well as lab-confirmed COVID-19 deaths.
Officials in some states have said they’ll adhere to the new CDC guidelines, but "each state has their own laws, which sometimes takes time," said Janet Hamilton, executive director Council of State and Territorial Epidemiologists (CSTE).
In mid-April, New York City released its first death count to include suspected -- not just lab-confirmed -- cases. That metric accounted for at-home deaths. The revised city figures, which added 3,700 deaths, drove up the nationwide death count by 17%.
Last week, scientists at Yale School of Public Health published a scholarly paper, which has yet to be peer-reviewed, that estimated that the actual death count in New York and New Jersey could be up to three times higher than the official tally of confirmed COVID-19 deaths or deaths that would be expected normally this time of year with respiratory diseases.
"Some states, such as Florida and Pennsylvania, might have missed deaths early on and might be under-counting deaths by a substantial degree currently," the Yale scientists concluded. "Other states, like Washington, have an accurate estimate of the mortality burden of the pandemic virus due to intense testing," the paper said. "And in states that have been hit hard by the pandemic virus, such as New Jersey and New York, the total excess mortality burden is 2-3 times that ascribed to COVID-19 in official statistics."
’The golden question’
Many U.S. states remain too overwhelmed by the outbreak or too short on supplies to perform postmortem COVID-19 testing.
Yet experts say localities’ inclusions of suspected cases in their death counts is vital going forward.
"It is critical to include both the probable and the confirmed cases so we have the full picture of the impact," said Hamilton, of CSTE. Failure to do so, she said, "would be a failure of our public health system."
Even those areas that can include probable and suspected COVID-19 deaths face challenges due to how little we yet understand about the disease, and how long the dead may carry it.
"Post-mortem, we don't know how long the [COVID-19 diagnostic] test is valid for after death," said CAP’s Williamson. "If a person is not found in their house for five days, does the COVID-19 test still work? We don't really know the answer to that."
There are two main types of death investigations in the U.S.: medical examiner autopsies and hospital-based autopsies.

Medical examiners are the most rigorously trained forensic pathologists in the death investigation field -- but even they do not have uniform national reporting protocols for COVID-19 deaths.
The CDC first introduced a common code to list COVID-19 as a cause of death on U.S. death certificates on March 24, followed by formal guidance on April 3, but the guidance will take time to take root nationwide, experts said.
Beyond a shortage of testing that is forcing hospital officials to prioritize testing of live patients over the deceased, many hospital pathologists remain wary of conducting autopsies during the pandemic because of all that is still unknown about the coronavirus, according to ABC News interviews around the nation.
Even swabbing the nose of a corpse could potentially re-introduce the virus into the air surrounding the body, pathologists said -- urging their colleagues to only conduct such testing in the proper settings.
One pathologist who spoke with ABC News on the condition of anonymity said a recurring theme online among prominent U.S. academic pathologists is that due to a limited, evolving understanding of how the virus spreads, shortages of personal protective equipment and limited autopsy rooms with appropriate precautions in hospitals, many pathologists "are scared to do the autopsies" for fear of being infected.
Yet postmortem samples and tissue can be preserved until more testing is available.
"You can freeze the nasal pharyngeal swabs and test them later," Aiken said. "And medical examiners and coroner's draw blood for toxicology. Eventually that blood could be used for antibody testing. So even though the lab tests are limited now, in the long run, they may be able to determine if deaths are COVID-19 related."
The final factor that undermines a complete COVID-19 death count, according to experts, is that many if not most of the people who have died had at least one additional underlying chronic medical condition that contributed to the deaths – particularly obesity, diabetes and hypertension.
But which factor actually caused the death?
"That’s the golden question: who died with COVID-19, and who died of COVID-19," Williamson concluded. "That’s what we still don’t know."
ABC News' Josh Margolin and Lee Ferran contributed to this report.
Related Topics

Trending Reader Picks
ABC News Live